Day 45 of the 100 Days Mission Ebola Clock (major update)
The 100 Days Mission (100DM) clock for Bundibugyo ebolavirus (BDBV) started on 18 May 2026, following WHO’s declaration of the outbreak as a public health emergency of international concern (PHEIC). Africa CDC declared a Public Health Emergency of Continental Security (PHECS) the following day.
Leading up to Day 100 on 25 August, we continue to provide updates every 15 days (alternating between minor and major updates) on the status and progress of BDBV diagnostics, therapeutics and vaccines (DTVs) availability and highlight immediate priority actions to ensure products can be rapidly evaluated, manufactured, deployed, and equitably accessed by affected communities.
On Day 45, we provide our latest major update on the status of BDBV diagnostics, therapeutics and vaccines. This update also includes a deep dive on the Expression of Interest (EOI) process for diagnostic candidates and the Emergency Use Listing (EUL) pathway and highlights the priority actions needed to ensure products can be rapidly evaluated, manufactured, and equitably accessed.
These updates are intended to support the work of partners and key initiatives and are developed in consultation with implementing partners of the 100DM. We are open to feedback on the accuracy of our data; please get in touch (info@ippsecretariat.org) if you have information to share.
The data used to inform this update has been collected through desk research using public information and direct updates from implementing partners of the 100DM.
Previous updates:
Rapid overview: Status of DTVs
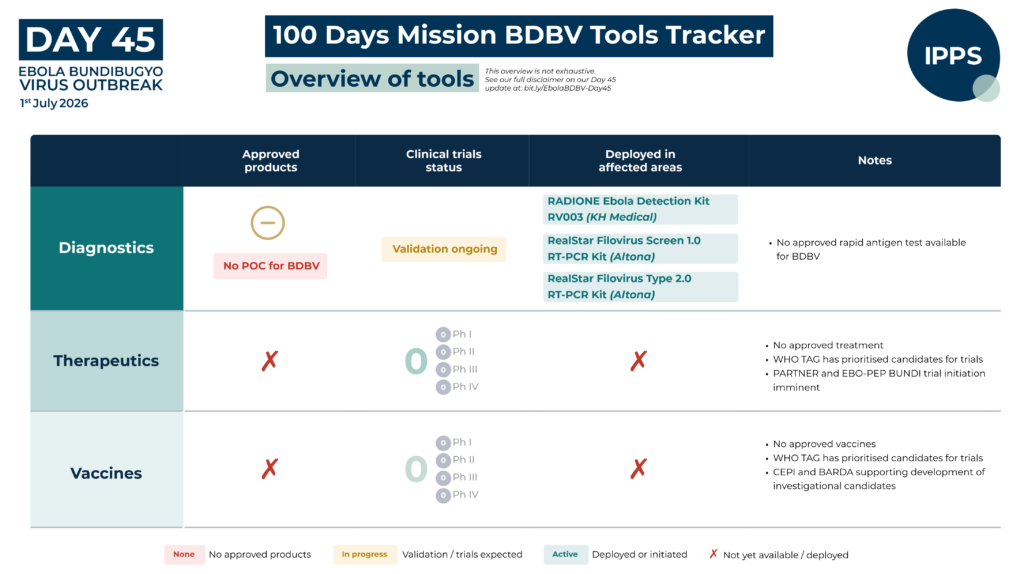
Diagnostics
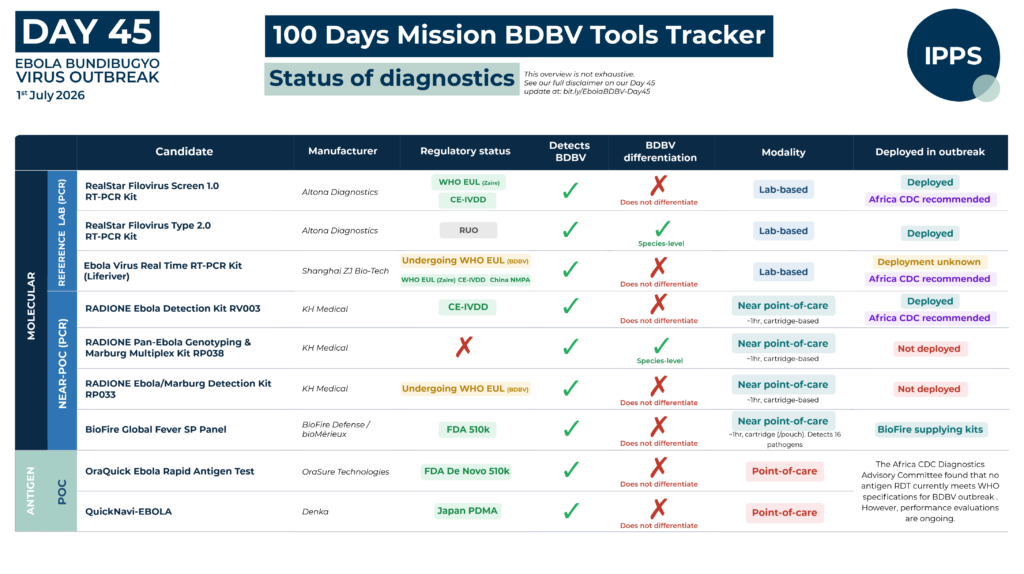
On Day 45, there are no approved point-of-care diagnostic tests specifically for Bundibugyo virus. The Xpert® Ebola test (Cepheid, USA), the near-point-of-care test (near-POC) routinely used in Ebola responses, does not detect BDBV, contributing to a significant detection delay in the early weeks of the outbreak. No Antigen Rapid Diagnostic Test (AgRDT) currently meets the specifications recommended by Africa CDC’s Diagnostics Advisory Committee for use in the current outbreak . Reference laboratory diagnosis continues to depend primarily on the Altona RealStar® Filovirus kits (Altona Diagnostics GmbH, Germany), while the RADI Ebolavirus Detection Kit on the RADIONE platform (KH Medical Co., Ltd., Republic of Korea) is the only near-POC molecular test operationally deployed, though availability remains severely constrained. Africa CDC has secured 100% of KH Medical’s current production capacity for RADIONE platforms, with technology transfer to Africa agreed to enable local manufacturing. Deployment to affected health zones is underway, although scaling up the number of RADIONE instruments available in the field remains a primary bottleneck for expanding testing.
Testing is currently being conducted across ten sites in the DRC, anchored by two reference laboratories, Institut National pour la Recherche Biomédicale (INRB), Kinshasa, and Laboratoire Rodolphe Mérieux (LRM), Goma. INRB researchers have published first field validation data comparing the RADIONE Ebola detection kit against the WHO-approved RealStar® Filovirus Screen RT-PCR kit in 148 samples from patients with suspected Ebola virus disease in Ituri province, demonstrating good agreement between the two assays.
A consortium of Africa CDC, WHO, PATH, and FIND, with support from Unitaid, received 83 eligible product submissions across four technology categories following the close of its Expression of Interest (EOI) on 11 June. Shortlisting has taken place, with selected candidates now entering analytical and usability studies; retrospective studies and prospective clinical field evaluations are expected to initiate shortly in the DRC and Uganda. Up to twenty laboratory-based molecular kits, eleven AgRDTs, and five near-POC molecular tests have been selected for evaluation (with discussions ongoing for a potential sixth test); no true POC molecular test has been selected to date. Additional details of selected candidates are provided in the diagnostics deep dive below.
The WHO EUL process for BDBV nucleic acid detection tests opened on 26 May, with six manufacturers currently invited to submit product dossiers. Further detail on the EUL process is provided in the diagnostics deep dive below.
As the evaluation process moves from shortlisting to scale-up, including procurement initiation, contracting, and protocol finalisation, complementary funding is still being sought to support key aspects of implementation.
Therapeutics
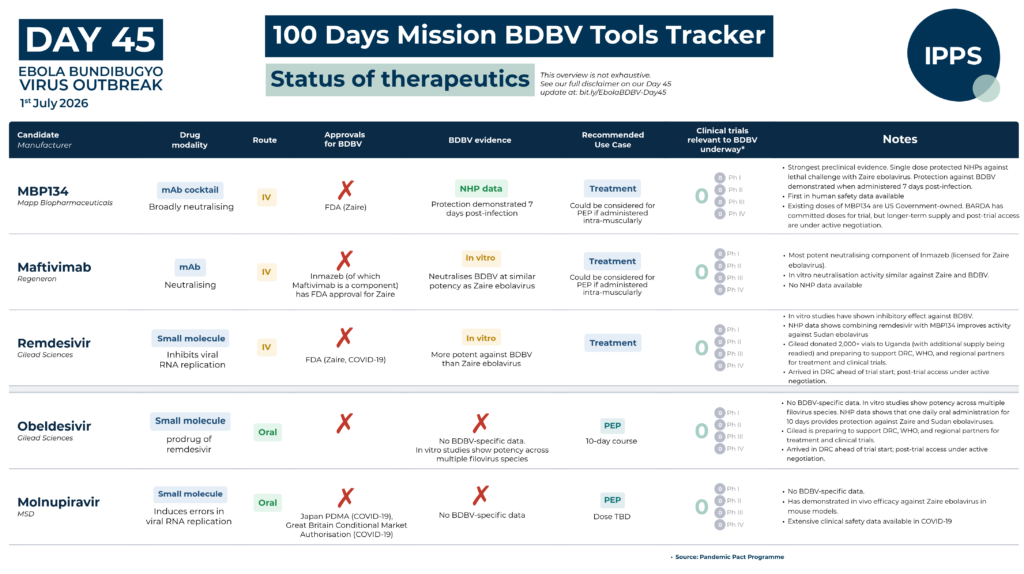
On day 45, there are no approved therapeutics for Bundibugyo virus disease. Existing licensed Ebola therapeutics – Inmazeb® and Ebanga® – are approved for Zaire ebolavirus only. A WHO Technical Advisory Group (TAG) has prioritised MBP134, maftivimab, and remdesivir for evaluation in clinical trials among confirmed cases, including investigation of combination therapy involving remdesivir and monoclonal antibodies. For post-exposure prophylaxis, obeldesivir has been prioritised. A separate TAG workstream is examining immunomodulatory and host-directed candidates; however, proper scientific evaluation of these agents for clinical trials requires generating BDBV-specific natural history data from patients – including immune markers, viral kinetics, coagulation status, and organ damage indicators – to determine appropriate timing of administration and patient selection, and to minimise the risk of detrimental effects.
The PARTNERS adaptive platform trial – developed by the University of Oxford and WHO – is testing MBP134, remdesivir, both drugs combined, or supportive care alone across four arms. The protocol has received regulatory and import authorisation in DRC and is expected to start imminently. The EBO-PEP BUNDI trial for post-exposure prophylaxis, co-led by INRB and ANRS, with support from WHO and Africa CDC, is evaluating obeldesivir and potentially molnupiravir as PEP candidates; the protocol has been amended, ethics approval obtained, and the trial is currently under regulatory review in DRC. This trial currently does not include children and pregnant women. No paediatric formulation of obeldesivir exists and there is insufficient evidence to guide safe dose adjustment of adult tablets – an urgent constraint given the age-specific mortality burden of BDBV. Addressing this will require either development of a paediatric formulation, pharmacokinetic studies to support dose adjustment, or identification of alternative oral antivirals with existing paediatric evidence.
On supply and access, remdesivir and obeldesivir – both supplied by Gilead Sciences – have arrived in DRC ahead of trial commencement; MBP134 (MAPP Biopharmaceutical) is expected to arrive imminently. Existing doses of MBP134 are owned by the US Government; BARDA has committed doses for the clinical trial, though longer-term supply and post-trial access commitments remain to be resolved. Gilead has announced a donation of more than 2,000 vials of remdesivir to Uganda under compassionate use and Monitored Emergency Use of Unregistered and Investigational Interventions (MEURI) frameworks to support the outbreak response, with additional supply being prepared for the DRC, WHO, and regional partners, including support for planned clinical trials; post-trial access planning is underway. Remdesivir has an existing African manufacturing base through EvaPharma in Egypt, and discussions on scaling production if trial results are favourable are ongoing. Ensuring that communities which contribute patients and data to clinical trials have guaranteed access to treatments if they prove effective is both an ethical imperative and an operational necessity – and one that must be resolved before, not after, trial results are available.
More broadly, while efforts such as Unitaid’s work on access pathways are under way, the wider ecosystem for therapeutics has yet to develop the dedicated financing and coordination infrastructure that exists for vaccines through mechanisms such as CEPI and Gavi. In the absence of equivalent structures – including advance purchase commitments, at-risk manufacturing financing, and post-trial procurement mechanisms – questions around timely, equitable and affordable access to successful candidates remain to be resolved.
Vaccines
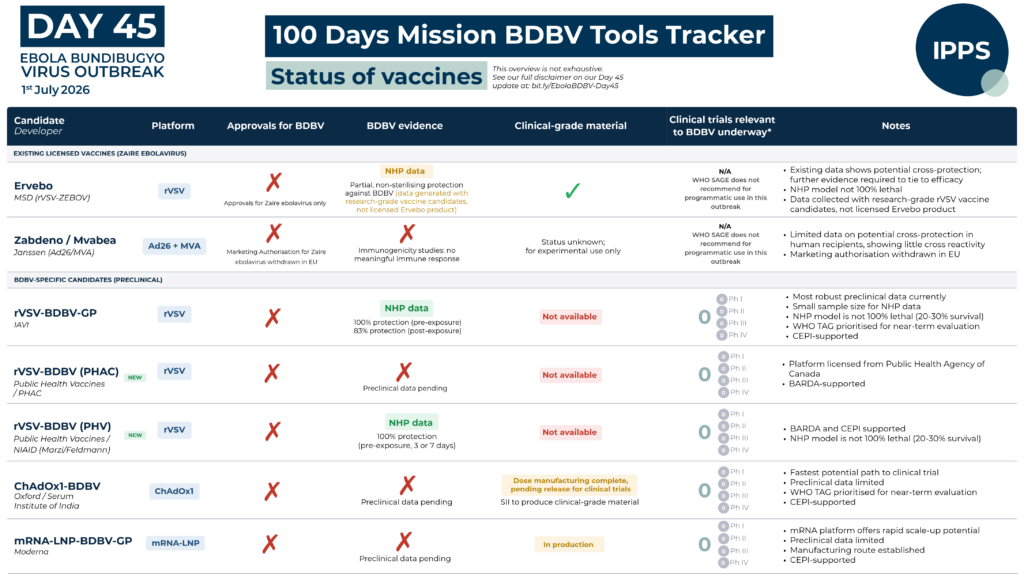
On day 45, there are no approved vaccines for Bundibugyo virus disease. The only licensed Ebola vaccine, Ervebo®, is indicated for Zaire ebolavirus only. WHO SAGE does not recommend Ervebo® for use outside controlled research settings in response to the current outbreak, in light of limited and inconclusive evidence on cross-protection of rVSV-vectored Zaire ebolavirus vaccines against BDBV.
The Bundibugyo-specific vaccine pipeline remains at an early stage, with no candidates yet available for deployment in clinical trials, and no Bundibugyo-specific vaccine expected to be available for near-term outbreak deployment. A WHO Technical Advisory Group (TAG) has prioritised two candidates for near-term evaluation: rVSV-BDBV-GP (IAVI), assessed as the most promising single-dose option for post-exposure use, and ChAdOx1-BDBV (Oxford University/Serum Institute of India), the first candidate to complete clinical-grade production – manufacturing of doses is now complete and pending release for clinical trials. CEPI is funding accelerated development of both prioritised candidates, including Master Virus Seed stock generation, clinical-grade manufacturing, and Phase 1 clinical trial preparation https://cepi.net/cepi-fast-tracks-three-bundibugyo-ebolavirus-vaccine-candidates. In addition, CEPI has committed up to $50 million to an mRNA-LNP candidate developed by Moderna, supporting preclinical testing, Phase 1 trials, and simultaneous manufacturing of doses at scale to enable Phase 2/3 trials to begin immediately if Phase 1 data supports progression. BARDA has additionally awarded funding to Public Health Vaccines for two further rVSV-vectored BDBV vaccine candidates – one developed in collaboration with the Public Health Agency of Canada, and a second based on research at NIAID, with CEPI co-funding Master Viral Seed stock generation for the latter https://www.phvaccines.com/downloads/Press%20Release-Jun-26.pdf.
CEPI’s calls for proposals – to advance early-stage BDBV candidates toward Phase 1 evaluation, and to support evidence generation through epidemiological modelling and assessment of cross-protection from existing ebolavirus vaccines – closed in June, with selections pending https://cepi.net/calls-for-proposals?selectedProposal=1779. CEPI’s request for information on Phase 1 clinical trial capacity across Africa, and BARDA’s request for project proposals under the BundiVx Programme https://www.rrpv.org/solicitation/bundibugyo-virus-outbreak-response-vaccines-bundivx/, also closed in June; outcomes are awaited. UNICEF and Gavi have issued a joint Expression of Interest seeking information from vaccine developers on plans to advance BDBV candidates through to licensure, with a view to establishing advance purchase commitments and supporting emergency dose availability, backed by Gavi’s $40 million First Response Fund allocation.
Immediate Priorities
– Sustain and strengthen the public health and clinical response as the foundation of outbreak control
- Surveillance and contact tracing, infection prevention and control, safe and dignified burials, high-quality clinical care, and risk communication and community engagement (RCCE) are the critical pillars of every Ebola response – and must be strengthened and sustained across all affected areas. Community trust and engagement are essential at every stage: for clinical care uptake, safe burials, contact tracing, clinical trial enrolment, and the eventual deployment of new medical countermeasures. Sustained engagement with local leaders, community figures, and health workers through culturally appropriate messaging must begin immediately.
– Scale diagnostic capacity and accelerate validation of new tools
- Expanding the number and throughput of testing sites and reducing sample transport times, while maintaining quality and biosafety standards, remain the most pressing operational priorities.
- Addressing operational gaps that continue to constrain diagnostic capacity – including ensuring continuity of reagent supply, biosafety deficiencies, infrastructure limitations (power, connectivity, equipment), and the need for additional trained laboratory technicians and sample collectors – requires targeted and sustained support from partners and funders.
- WHO has opened an Emergency Use Listing (EUL) procedure for nucleic acid detection tests for Bundibugyo virus disease. Manufacturers should apply through the EUL questionnaire and should also be encouraged to pursue other regulatory pathways in parallel of performance evaluation efforts.
- Diagnostic validation efforts should be prioritised as planned and financially supported as needed. Following selection of candidates through the coordinated EOI process, performance evaluations of molecular and antigen-based diagnostics must be completed as rapidly as possible, with results feeding into EUL submissions and Africa CDC Diagnostics Advisory Committee recommendations
- Development and validation of point-of-care solutions, including AgRDTs, remains a critical priority for decentralised and community-level testing.
- Comprehensive mapping of laboratory capacity across affected and at-risk countries should continue, with results shared across partners in real time to identify gaps and maximise diagnostic accessibility.
- Partners engaged in diagnostic, WASH supplies, PPE and laboratory consumables procurement should actively participate in the central WHO-hosted procurement dashboard to ensure efforts are not duplicative and to provide real-time visibility on supply chains and gaps.
- Responsibility for ensuring that diagnostic tools for BDBV – particularly point-of-care tests – are developed, funded, validated, and deployed at scale requires active coordination and financing commitments from partners and funders. WHO is coordinating these efforts through the iMCM‑Net Diagnostics workstream, with weekly meetings open to all interested partners.
– Initiate clinical trials and secure post-trial access commitments for therapeutics
- Any remaining operational barriers to enrolment in both the PARTNERS adaptive platform trial and EBO-PEP BUNDI must be removed urgently, including finalising site readiness, cold chain, and logistics.
- Trial protocols must be designed to enable the inclusion of children and pregnant women where feasible. Filovirus disease has historically been associated with severe outcomes in both groups, and their exclusion risks leaving them without an evidence base for treatment and post-exposure prophylaxis. Current constraints on paediatric dosing of candidate antivirals must be urgently addressed through development of paediatric formulations, pharmacokinetic studies on dose adjustment of adult tablets, or identification of alternative options for existing paediatric dosing.
- Post-trial access commitments must be secured before trial results are available – including timely, equitable, and affordable access, in-country registration in DRC, Uganda, and neighbouring at-risk countries, and clarity on indemnification and compensation arrangements for trial participants and post-deployment use. Unitaid, with the Medicines Patent Pool and CHAI, is developing access roadmaps to clarify roles and responsibilities across the value chain for post-trial access and longer-term availability.
- Financing for at-risk manufacturing – particularly where lead times are long and decisions must precede efficacy data – must be clarified and committed now.
– Accelerate vaccine development and define the full pathway to access
- For lead vaccine candidates, immediate action must focus on production of clinical-grade material and completion of preclinical requirements to enable Phase 1 trials without delay. Access to ferrets and nonhuman primates is limited; coordination on prioritisation and sequencing of preclinical studies will be essential to avoid delays.
- Trial protocols to be conducted in outbreak settings should be designed to enable inclusion of children and pregnant women at the earliest appropriate stage, including through consideration of parallel/rapid Ph2 studies in special populations. Filovirus disease has historically been associated with severe outcomes in both groups, and building an evidence base for these populations is essential to ensure that any licensed vaccine can be equitably deployed.
- Responses to CEPI’s calls for proposals on Phase 1 candidate advancement and evidence generation, CEPI’s request for information on African Phase 1 trial capacity, and BARDA’s BundiVx Programme call for VSV-platform candidates – all closed in late June – must be rapidly assessed to inform further candidate prioritisation and operational trial planning.
- Vaccine developers should respond to UNICEF and Gavi’s joint Expression of Interest on licensure pathways and manufacturing scale up. Information gathered will inform the design of advance purchase commitments and support emergency dose availability, backed by Gavi’s $40 million First Response Fund allocation.
– Sustain regulatory momentum and operational coordination
- The collaboration between AMA, African regulatory authorities, WHO PQ, and EMA’s Emergency Task Force on regulatory pathways and EUL processes must be sustained to ensure medical countermeasures can be rapidly registered and deployed in affected and at-risk countries.
- Close coordination between affected governments, WHO, Africa CDC, regulators, procurers, and implementing partners remains essential to ensure financing and response tools can be deployed quickly and equitably.
Diagnostics Deep Dive: Evaluating Bundibugyo Diagnostics
Timely and accurate diagnosis is the foundation of effective outbreak control. It enables rapid case identification, isolation, and contact tracing – the essential chain that interrupts transmission. The diagnostic response to the current Bundibugyo virus outbreak reflects a critical structural gap. Early detection delays were driven in part by the inability of the Xpert Ebola Assay – used on widely deployed GeneXpert® systems and designed for Zaire ebolavirus – to detect Bundibugyo virus. This is not a flaw specific to one test, but symptomatic of a wider, systemic issue: any test optimised to detect a single pathogen will always be vulnerable to being outpaced by the next unanticipated one, pointing to a broader need for pan-species and multiplex diagnostic tools to support both outbreak preparedness and sustainability, with syndromic coverage to differentiate filovirus infection from other causes of febrile illness representing an added benefit. In the immediate term, the priority remains securing reliable BDBV-specific detection capacity, particularly at the point of care, to support the current response; in the longer term, investment in such platforms will be essential to deliver on that broader goal. The remainder of this section assesses how current and emerging tools, across the full diagnostic cascade, are being evaluated for the immediate outbreak need.
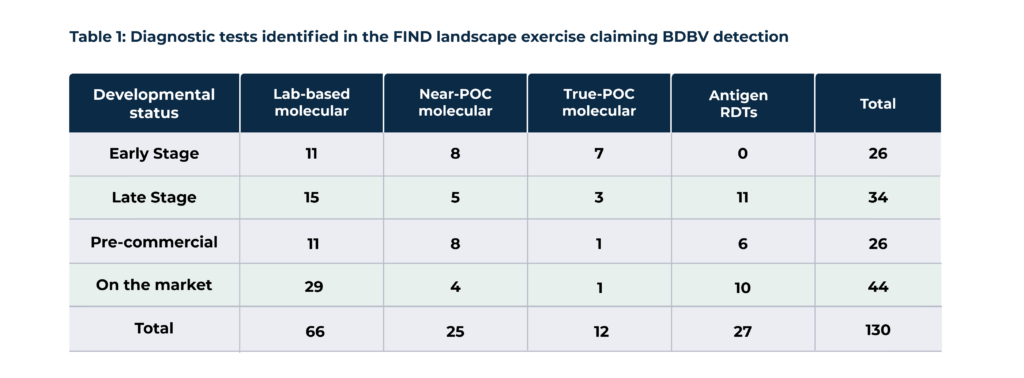
The latest diagnostic landscape compiled by FIND (as of 17 June) identified 130 tests across molecular assays and antigen RDTs at various stages of development claiming BDBV detection. These include 66 laboratory-based molecular tests, 25 near-POC molecular tests, 12 true POC molecular tests, and 27 antigen RDTs (Table 1). While at least half of the tests in most technology categories are either commercially available or in the pre-commercial phase, true POC molecular solutions with potential to enable further decentralisation to the community level remain scarce, with the majority still in early-stage development.
Despite the apparent breadth of available platforms, independent, rigorous evaluation across the full diagnostic cascade is required to assess suitability for BDBV detection, from reference laboratory to community level. Addressing this evaluation gap – for the current outbreak and for future readiness – requires systematic assessment of all platforms now available or close to market entry. This includes not only molecular platforms but also antigen-based rapid diagnostic tests, which remain an unmet need for BDBV and have the potential to be transformative for community-level decision-making.
To this end, a consortium comprising Africa CDC, WHO, PATH, and FIND, with support from Unitaid, launched a coordinated Expression of Interest (EOI) on 5 June 2026 , inviting manufacturers of laboratory-based molecular kits, point-of-care molecular tests, and AgRDTs to participate in independent performance evaluations. The EOI closed on 11 June, with shortlisting completed on 24 June. The EOI drew a strong response, with 83 eligible submissions received, representing 80% of the tests identified in the FIND landscape that have reached at least late-stage development, indicating broad engagement from manufacturers active in the space and suggesting that independent evaluation will cover the substantial majority of tests with realistic near-term potential for deployment. Evaluation partners include the Hôpitaux Universitaires de Genève (HUG), Charité – Universitätsmedizin Berlin, Bernhard Nocht Institute for Tropical Medicine (BNITM), United Kingdom Health Security Agency (UKHSA), INRB, Uganda Central Public Health Laboratories (CPHL) and PATH.
Tests in all technology categories were selected through a structured, multi-stage review process led by WHO, Africa CDC, FIND, PATH, and Unitaid with support from CHAI. The assessment incorporated criteria including technical performance, usability and workflow, suitability for intended use settings, product readiness, availability and affordability, and organisational maturity. Eligible tests were required to be commercial or near-commercial products, able to supply at least 2,000 assay kits and five devices within 15 days, and committed to transparent and affordable pricing for low- and middle-income countries. Tests proprietary to a single instrument (for laboratory-based molecular kits), prototypes not yet design-locked, and those not available for supply within three months in the DRC and neighbouring countries were excluded.
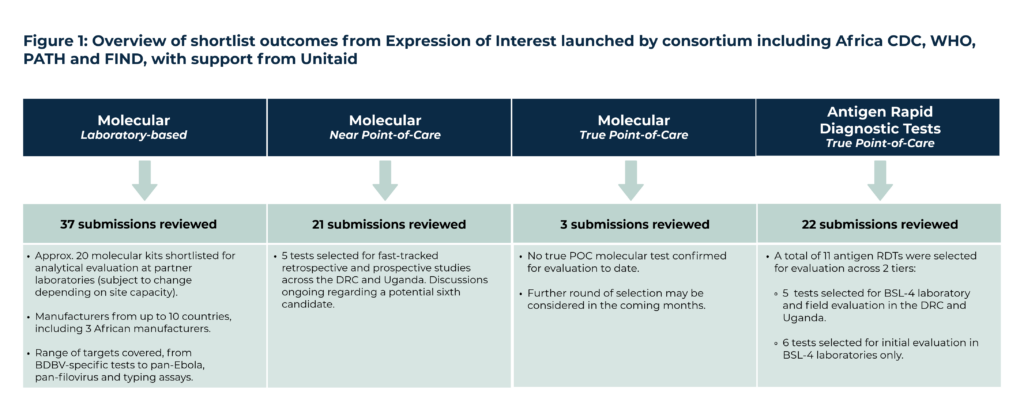
This section describes the tests selected for evaluation across each category (Fig 1). Candidates were assessed against a structured set of quantitative and qualitative criteria covering technical performance, usability, operational fit, and supply readiness, among others. While the evaluation spans the full diagnostic cascade, priority has been given to near point-of-care and true point-of-care tests, reflecting the urgent operational need for decentralised testing solutions in the affected areas. Further detail on the evaluation framework is provided at the end of this section.
Molecular – Laboratory-based
Reference laboratory-based PCR assays remain the gold standard for Ebola diagnosis and the anchor of any confirmatory testing system. These assays work by extracting viral RNA from a patient sample and amplifying specific genetic sequences of the target pathogen, enabling highly sensitive and specific detection even at low viral loads. They are run on standard PCR laboratory equipment by trained laboratory technicians, and can deliver results within two to three hours. While they require conventional laboratory infrastructure – including reliable power, cold chain for reagents, and biosafety-compliant facilities – their sensitivity and specificity make them the reference point against which all other diagnostic modalities are benchmarked, and they remain an essential component of the diagnostic system regardless of what decentralised tools are deployed alongside them.
For the purposes of this evaluation, eligible tests were required to detect Bundibugyo virus -either as a species-specific target or as part of a broader pan-orthoebolavirus assay, with species differentiation considered an additional advantage. Detection of Marburg virus and other haemorrhagic fever viruses was regarded as an added advantage where available. Tests were required to deliver results within three hours, and lyophilised reagents were considered advantageous because they eliminate cold-chain dependencies.
In the current outbreak, reference laboratory diagnosis has depended primarily on the Altona RealStar® Filovirus kits. Reliance on kits from a single manufacturer represents a meaningful vulnerability – both in terms of supply security and the ability to cross-check discordant results. The evaluation process will enable a broader set of molecular laboratory kits to be assessed under standardised conditions, generating the performance data needed to expand the options available to reference laboratories in affected and at-risk countries.
EOI outcomes to date:
Following a review of 37 submissions, representing more than half of the lab-based molecular tests identified in FIND’s landscape, approximately 20 molecular kits were shortlisted for analytical evaluation at partner laboratories using extracted BDBV RNA, though the final number may be subject to changes as the list is still being finalised. The selected assays represent manufacturers from up to ten countries, including three African manufacturers (South Africa, Nigeria and Egypt), and cover a wide range of targets – from BDBV-specific tests to pan-Ebola, pan-filovirus, and genotyping assays.
Molecular – Near-Point-of-Care
Near-POC molecular tests occupy a critical position in the diagnostic cascade: they extend sensitive molecular testing beyond the reference laboratory to intermediate-level facilities – district hospitals and referral centres – that are closer to affected communities but retain some laboratory infrastructure and technical capacity. In the current outbreak, where affected areas are often remote and sample transport to reference laboratories can take several days, the ability to deliver molecular results at district level is not just operationally convenient but essential to timely case identification and response. These platforms are typically cartridge-based, integrating the key steps of nucleic acid extraction, amplification, and detection within a single sealed cartridge, removing the need for the multiple manual preparation steps and specialist equipment that conventional PCR requires. This makes them accessible to healthcare workers with limited laboratory training, and capable of delivering results within ~90 minutes.
For the purposes of this evaluation, eligible tests must detect BDBV as for the laboratory-based category, with species differentiation or pan-species coverage, and additional coverage of Marburg virus and other haemorrhagic fever viruses considered added advantages. Results must be available within 90 minutes. Tests must require minimal pre-test processing (sample inactivation or transfer steps only), no centrifugation, and no precise measurement of reagents or samples.
The RADI Ebolavirus Detection Kit on the RADIONE platform (KH Medical) is the only near-POC molecular test currently deployed operationally in the outbreak; the evaluation will assess additional candidates alongside it, generating performance data to guide procurement and deployment decisions
EOI outcomes to date:
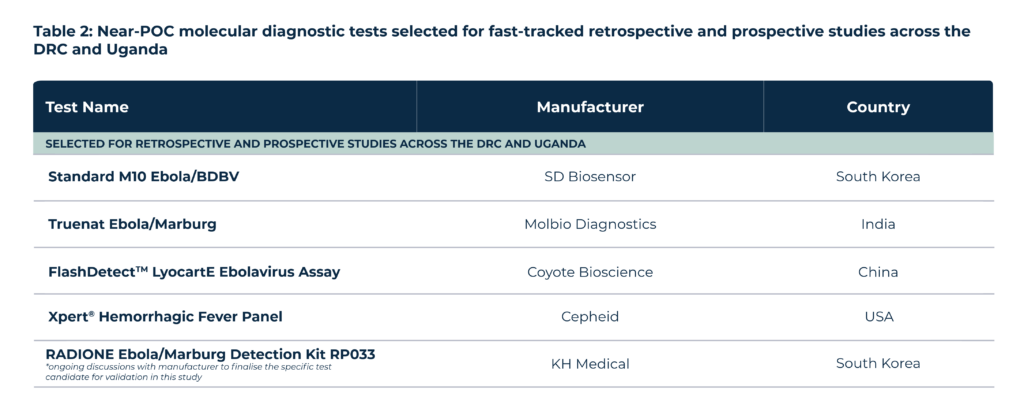
Following a review of 21 submissions, covering the majority of the near-POC molecular tests identified in FIND’s landscape (21 out of 25), five tests were selected for fast-tracked retrospective and prospective studies across the DRC and Uganda, with discussions ongoing regarding a potential sixth candidate (Table 2).
Molecular – True Point-of-Care
True point-of-care molecular tests represent the most decentralised form of molecular diagnostics: handheld or portable devices capable of delivering molecular results at primary health facilities, community health posts, and in the field. These platforms employ diverse nucleic acid amplification technologies – including conventional PCR on portable, battery-operated devices, as well as isothermal amplification methods such as LAMP, which eliminate the need for thermal cycling – designed for use by non-laboratory-trained health workers or community workers.
For evaluation purposes, eligible tests must detect BDBV as for the laboratory-based category, with species differentiation and additional coverage of Marburg virus and other haemorrhagic fever viruses considered added advantages; require minimal pre-test processing (sample inactivation or transfer steps only), no centrifugation, and no precise measurement of reagents or samples; and operate on battery power or portable charging across a wide temperature and humidity range. Results must be available within 90 minutes.
In the DRC context, where terrain, insecurity, and infrastructure constraints mean that even district-level facilities are inaccessible to some affected communities, the ability to deliver molecular results without any laboratory infrastructure at all, provided that safety standards are met, could fundamentally extend the reach of the diagnostic response beyond what near-POC testing alone can achieve.
No true POC molecular test for BDBV is currently available for deployment in the outbreak.
EOI outcomes to date:
Three submissions were reviewed; no true POC molecular test has been confirmed for evaluation to date, reflecting a lack of readiness in this technology category as shown in FIND’s landscape, largely driven by the challenges associated with blood sample processing. A further round of selection may be considered in the coming months.
Antigen Rapid Diagnostic Tests (AgRDTs) – True Point-of-Care
AgRDTs detect viral proteins directly through lateral flow immunoassays, enabling results in under 30 minutes from specimen types compatible with decentralised testing, including whole blood or buccal/oral samples, with no equipment, laboratory infrastructure, or specialist training required. They are typically read visually by the naked eye, though some may use portable, battery-operated readers where this improves performance, making them deployable at the community level – the lowest tier of the health system – by non-laboratory-trained healthcare workers or community workers. AgRDTs do not require cold-chain management, a significant operational advantage in resource-limited settings with constrained logistics infrastructure
In an outbreak context, AgRDTs have the potential to dramatically accelerate case identification and isolation decisions – deployable at a cost, scale and speed that molecular testing, however decentralised, cannot match. This is particularly relevant for contact tracing, where the volume of contacts requiring follow-up is less easily met by device-dependent testing alone. However, they typically offer lower sensitivity than molecular assays, particularly early in infection when viral antigen loads may not yet be detectable. AgRDTs can also play a critical role in screening recently deceased individuals to inform safe and dignified burial practices. In this use case, viral loads may be high, mitigating concerns of low sensitivity.
For the purposes of this evaluation, eligible tests must at minimum detect Bundibugyo virus, with pan-Orthoebolavirus inclusivity and Orthomarburgvirus detection considered added advantages. Results must be available within 30 minutes. In the current outbreak, the Africa CDC Diagnostics Advisory Committee reviewed available evidence on antigen RDTs for BDBV against the WHO Target Product Profile for Ebola diagnostics and concluded that no AgRDT currently meets the required specifications for recommendation. This is an acknowledged gap: a high-performing, validated AgRDT for BDBV would materially change the operational reach of the diagnostic response.
EOI outcomes to date:
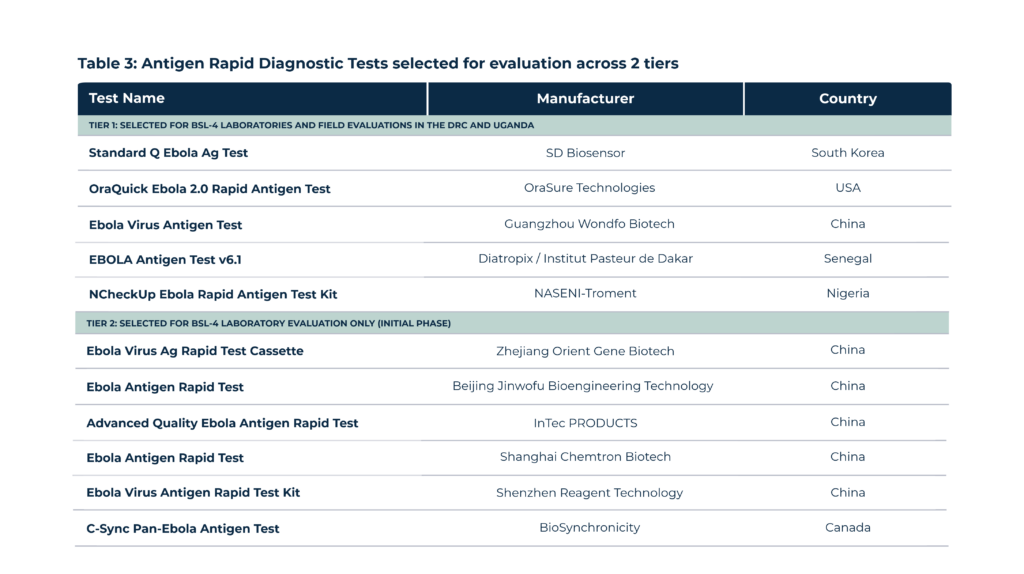
Following a review of 22 submissions (out of 27 identified in FIND’s landscape), 11 antigen RDTs were selected for evaluation across two tiers (Table 3).
Evaluation Framework and Next Steps
The evaluation will be conducted through a combination of parallel analytical and clinical studies, depending on the technology category. Analytical and usability assessments will generate data on limit of detection, specificity, and user workflow, while selected technologies simultaneously undergo retrospective and prospective clinical evaluations in DRC and Uganda. Near-POC platforms, identified as a high priority, are being fast-tracked directly into field evaluations. For antigen RDTs, a subset of tests has been prioritised for field evaluation in the DRC and Uganda, alongside complementary analytical testing in BSL-4 laboratories to generate limit of detection data using live virus titration; this BSL-4 work has been extended to an additional six AgRDTs. Planning for field evaluations is underway, with support from Unitaid and implemented by INRB, CPHL, Africa CDC, WHO and PATH. The study will include retrospective testing initially with plans to transition to prospective testing and include an adaptive design, with regular interim analyses planned. This will facilitate rapid data availability.
The evaluation is designed to generate robust, independent evidence to inform national and regional decision-making, including potential recommendations by Africa CDC, and to support manufacturers for WHO Emergency Use Listing submissions or other regulatory pathways. Neither selection nor participation constitutes endorsement by any consortium or evaluation partner or guarantee of regulatory approval; however, data generated will be directly relevant for EUL dossier preparation and broader policy uptake.
WHO Emergency Use Listing (EUL) procedure
WHO opened its EUL procedure for in vitro diagnostics for Bundibugyo virus nucleic acid detection on 26 May 2026, with instructions and requirements for EUL submissions published three days later. The EUL process provides a time-limited, risk-based pathway for regulatory authorisation: evaluation determines whether submitted data demonstrate a reasonable likelihood that a product’s quality, safety, and performance are acceptable and that the benefits outweigh the foreseeable risks in the context of a PHEIC. The process has attracted significant manufacturer interest: 30 manufacturers made contact, 25 submitted the product questionnaire covering 36 kits, and 6 manufacturers covering 8 IVDs have now been invited to submit full product dossiers. Of these, two products are currently under active dossier and quality management system review: the RADIONE Ebola/Marburg Detection Kit (KH Medical, South Korea) and the Ebola Virus Real Time RT-PCR Kit (Shanghai ZJ Bio-Tech, China). The status of all active applications is publicly available on the WHO prequalification website. Pre-submission calls are ongoing.
Calls for Expression of Interest and Proposals
Diagnostics
WHO Emergency Use Listing (EUL) for nucleic acid detection tests: Manufacturers should submit expressions of interest through the EUL questionnaire. Formal submission instructions and requirements for manufacturers seeking EUL approval for in vitro diagnostics detecting Bundibugyo virus nucleic acids.[related to current response]
Therapeutics
Development of monoclonal antibody therapeutics for prevention and treatment of filoviral and related emerging viral infections (Deadline 13 April 2027) [early stage]
Vaccines
UNICEF and Gavi joint Expression of Interest on BDBV vaccine licensure pathways and manufacturing scale-up (Deadline 10 July 2026) [related to current response]
EU investigational filovirus vaccine reserve tender: the European Commission is seeking to establish and maintain an investigational reserve of candidate vaccines against Ebola Sudan, Bundibugyo, and/or Marburg viruses for rapid deployment in outbreak-associated clinical trials. (Deadline 2 September 2026) [related to current response]
Acknowledgements
The diagnostics deep dive in this update draws extensively on data and insights provided by FIND, WHO and Africa CDC. We are also grateful to the Pandemic Pact Programme, PATH, CEPI, IFPMA, Gilead, Roche, MSD, MSF, Unitaid, PANTHER Health, Intrepid Alliance, i-MCM-Net Secretariat, Wellcome, Institut Mérieux and Airfinity for additional data, verification, and critical feedback to this tracker.
If you have additional updates or information you would like to see reflected in future iterations, please contact us at info@ippsecretariat.org.
Disclaimer for the Ebola Bundibugyo MCM Tools Tracker
Data shown in the tracker is not exhaustive. It prioritises candidates assessed by WHO TAG, actively discussed in partner coordination meetings and working groups, recommended by Africa CDC, and currently deployed or under evaluation. Additional products and updates will be integrated as they emerge and as existing candidates progress through development and evaluation.