Day 15 of the 100 Days Mission Ebola Clock
On 17 May 2026, WHO declared the Ebola outbreak caused by Bundibugyo virus (BDBV) in the Democratic Republic of Congo (DRC) and Uganda a Public Health Emergency of International Concern (PHEIC). This declaration marked the start of the 100 Days Mission clock, and the IPPS published a statement on the state of Diagnostics, Therapeutics and Vaccines (DTVs) at Day 0. Africa CDC followed on 18 May 2026, declaring the outbreak a Public Health Emergency of Continental Security (PHECS), acting on the recommendations of its Emergency Consultative Group (ECG).
Current evidence suggests that this is a novel spillover event from the animal reservoir, distinct from previous Bundibugyo outbreaks. A critical detection gap exists because GeneXpert®, the most commonly used frontline tool in this outbreak response, detects Zaire but not Bundibugyo ebolavirus. This has substantially delayed case confirmation and isolation. Cross-border spread to Uganda has been confirmed, with heightened risk of further transmission to Rwanda and South Sudan. For detailed epidemiological updates, see WHO situation reports at https://www.afro.who.int/health-topics/disease-outbreaks/ebola-who-african-region
Leading up to Day 100 on 25 August 2026, we will provide regular updates on the status and progress of Bundibugyo ebolavirus DTV availability and highlight specific priority actions to ensure products can be rapidly evaluated, manufactured, deployed, and equitably accessed by affected communities. These updates are intended to support the work of partners and key initiatives such as WHO’s i-MCM-net and R&D Blueprint (with overview over Technical Advisory Groups and Collaborative Open Research Consortia (CORCs).The data used to inform this update has been collected through desk research using public information and direct updates from implementing partners of the 100 Days Mission. Please find the latest updates at https://ippsecretariat.org/news/
Rapid overview: Status of DTVs
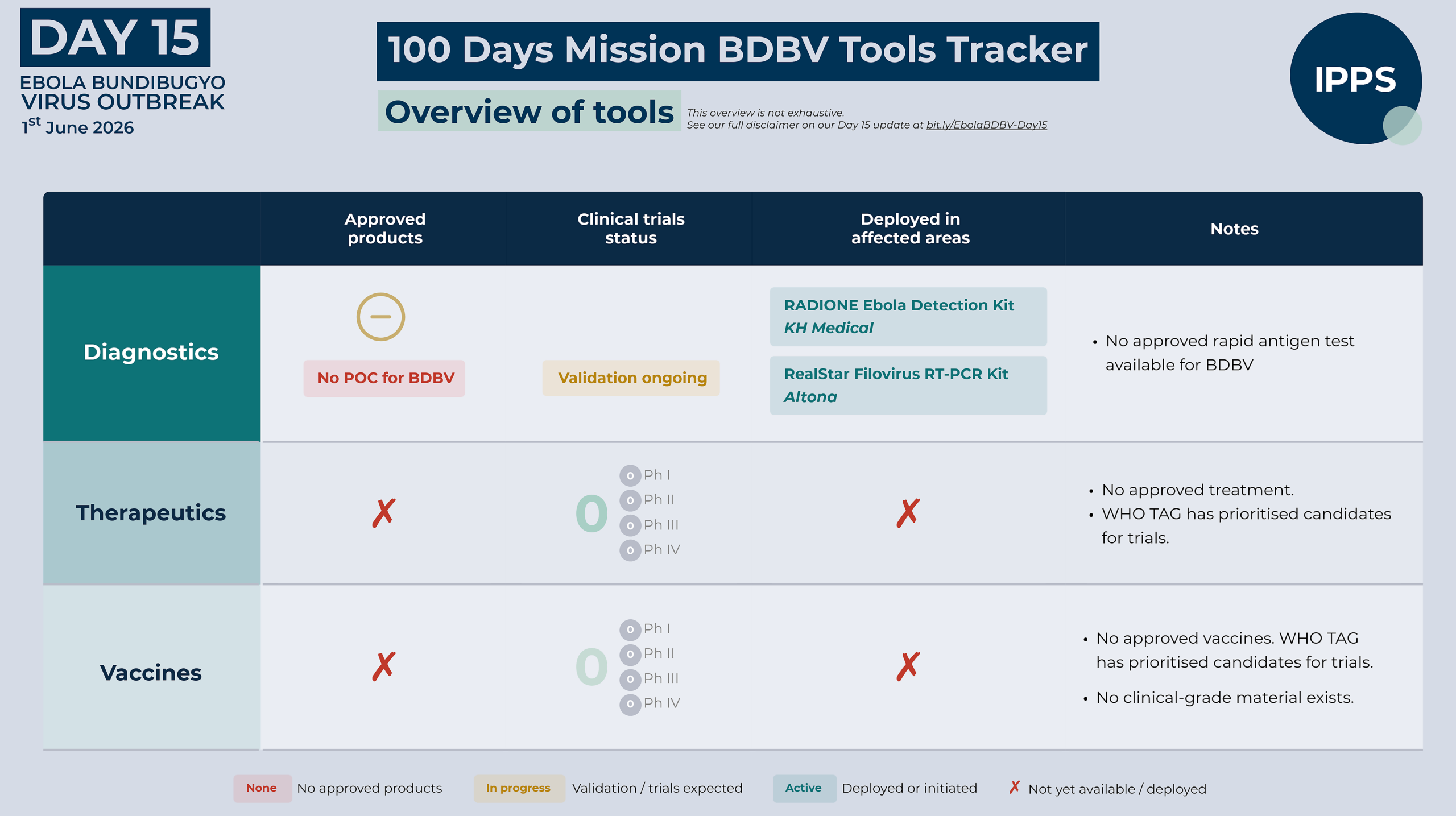
Diagnostics
On Day 15, there are no approved point-of-care diagnostic tests specifically for Bundibugyo virus. Pan-filovirus assays such as the Altona RealStar Filovirus Screen are being used for diagnosis in reference laboratories, but are not readily available in decentralised locations, substantially delaying case confirmation and isolation. The KH Medical RADIONE Ebola Detection (RADI) kit is currently the only deployed near-point-of-care molecular test that detects Bundibugyo. The GeneXpert® platform – the near-point-of-care test routinely used in Ebola responses – does not detect Bundibugyo virus.
To accelerate diagnostic availability, WHO has opened its Emergency Use Listing procedure for nucleic acid detection tests. To support candidate validation, a BDBV diagnostics validation framework is being prioritised, with the support of Unitaid, under the leadership of the joint Africa CDC and WHO continental Incident Management Support Team (IMST), in collaboration with PATH, FIND, with an expression of interest to follow shortly.
Therapeutics
On Day 15, there are no approved therapeutics for Bundibugyo virus disease. Existing licensed Ebola therapeutics – Inmazeb and Ebanga – are approved for Zaire ebolavirus only. However, a WHO Technical Advisory Group (TAG) has completed a rapid prioritisation review identifying promising candidates for both treatment and post-exposure prophylaxis (PEP). Among, investigational medical countermeasures, PEP currently represents the most immediately deployable preventative measure, pending the clinical availability of Bundibugyo-specific vaccine candidates.
For treatment, prioritised candidates include the pan-ebolavirus monoclonal antibody cocktail MBP134 and maftivimab, alongside the antiviral remdesivir, including potential combination therapy approaches. For post-exposure prophylaxis, obeldesivir – an oral antiviral offering significant operational advantages – has been prioritised. Clinical trials, including the PARTNERS adaptive platform trial co-developed by ISARIC for treatment and the EBO-PEP BUNDI trial sponsored by ANRS for post-exposure prophylaxis, are expected to begin shortly.
Vaccines
There are no approved vaccines for Bundibugyo virus disease. Until recently, two vaccine regimens were licensed for Zaire ebolavirus: Ervebo®, and the Zabdeno®/Mvabea® two-dose regimen, which had its European Commission marketing authorisation withdrawn in May 2026. Ervebo®, now the only licensed Ebola vaccine, is indicated for Zaire ebolavirus only and is not licensed for prevention of Bundibugyo virus disease; evidence on cross-protection to other Ebola virus species remains limited and inconclusive. WHO Strategic Advisory Group of Experts on Immunization (SAGE) does not recommend Ervebo® for use outside of controlled research settings in response to the current outbreak.
Several unapproved Bundibugyo-specific candidates exist at various stages of pre-clinical development. A WHO Technical Advisory Group (TAG) has prioritised two candidates for near-term evaluation: rVSV-BDBV-GP (IAVI) and ChAdOx1-BDBV (Oxford/Serum Institute of India). However, none of these candidates are currently available in clinical-grade form, and based on current timelines, no Bundibugyo-specific vaccine is expected to be available for near-term outbreak deployment. CEPI is funding rapid development of these prioritised candidates alongside an mRNA-LNP vaccine by Moderna, and has opened a Call for Proposals to evaluate additional promising options.
A detailed assessment of diagnostic, therapeutic, and vaccine candidates is provided further below.
Immediate Priorities
Sustain and strengthen the public health and clinical response as the foundation of outbreak control
- Surveillance and contact tracing, infection prevention and control, safe and dignified burials, high-quality clinical care, and risk communication and community engagement (RCCE) are the critical pillars of every Ebola response – and must be strengthened and sustained across all affected areas. Community trust and engagement are essential at every stage: for clinical care uptake, safe burials, contact tracing, clinical trial enrolment, and the eventual deployment of new medical countermeasures. Sustained engagement with local leaders, community figures, and health workers through culturally appropriate messaging must begin immediately.
Scale diagnostic capacity to affected communities and validate new tools
- Immediate efforts must focus on expanding access to sensitive RT-PCR diagnostics and near point-of-care testing. This includes rapidly scaling deployment of Altona RT-PCR kits to reference laboratories in affected health zones, and accelerating the delivery and operationalisation of RADI kits and associated machines to decentralised locations. Head-to-head validation of these assays must proceed in parallel.
- WHO has opened an Emergency Use Listing (EUL) procedure for nucleic acid detection tests for Bundibugyo virus disease. Manufacturers should submit expressions of interest through the EUL questionnaire.
- Development of point-of-care diagnostics remains a critical priority; rapid EUL pathways for promising candidates should be established to enable decentralised testing and community-level decision-making.
- FIND is conducting an expression of interest process to identify available and near-ready diagnostic solutions. Manufacturers with candidate diagnostics should participate.
- Comprehensive mapping of laboratory capacity across affected regions in the DRC and Uganda is critical, with the objective of maximising near point-of-care diagnostic accessibility and operational capacity.
- Partners engaged in diagnostic, WASH supplies, PPE and lab consumables procurement should actively participate in the central WHO-hosted procurement dashboard to ensure efforts are not duplicative and to provide real-time visibility on supply chains and gaps
..
Rapidly initiate clinical trials for investigational therapeutics and vaccines, and advance new candidates
- Randomised controlled trials evaluating candidate therapeutics should begin as quickly as possible. The PARTNERS adaptive platform trial for treatment candidates and the EBO-PEP BUNDI trial for post-exposure prophylaxis must commence without delay, with enrolment in affected areas and protocols designed to generate rapid, actionable efficacy and safety data.
- Access for affected areas post-trial must be planned now, not deferred until efficacy is demonstrated (access is not an afterthought). Unitaid, with the Medicines Patent Pool and CHAI, is mapping access pathways and identifying market gaps to ensure therapeutic availability.
- For lead vaccine candidates, immediate action must focus on production of clinical-grade vaccine material where it does not currently exist. Concurrently, acceleration of preclinical data generation to support regulatory decisions must proceed. Priority areas for evidence generation should be defined with tiered requirements based on platform maturity and prior knowledge. Trial protocols and operational planning should be prepared in parallel to enable rapid initiation once regulatory and preclinical requirements are met.
- CEPI has launched a Call for Proposals to advance early-stage BDBV vaccine candidates toward Phase 1 evaluation. Developers with scientifically robust candidates on credible pathways to clinical trials are encouraged to apply.
Accelerate regulatory harmonisation and operational coordination
- Regulatory coordination, particularly through the African Medicines Agency, will be essential to ensure investigational products can move rapidly to affected communities.
- Close coordination between affected governments, WHO, Africa CDC, regulators, procurers, and implementing partners will also be critical to ensure financing and response tools can be deployed quickly and effectively. There is a critical need for continued coordination between diagnostics, vaccines, and therapeutics stakeholders.
Deep Dive: Status of DTVs
The medical countermeasures described in this section are not an exhaustive inventory of all products in development globally. Rather, they represent the candidates currently identified as leads for the response – those assessed by WHO TAG, actively discussed in partner coordination meeting, recommended for use by Africa CDC, and currently deployed or under evaluation. As new products emerge and existing candidates progress through development and evaluation, this landscape will continue to evolve.
Diagnostics
On Day 15, there are no approved point-of-care diagnostic tests specifically for Bundibugyo virus. In the absence of a Bundibugyo-specific RT-PCR, pan-filovirus assays such as the Altona RealStar Filovirus Screen are currently being used for diagnosis in reference labs, but are not readily available in decentralised locations across the affected area. This poses a particular challenge in DRC, due to challenging terrain and infrastructure, and ongoing conflict. The GeneXpert® platform – the near-point-of-care test routinely used in Ebola responses – cannot detect Bundibugyo virus. Initial testing at the Provincial Public Health Laboratory in Bunia using GeneXpert® returned negative results on samples that subsequently tested positive by pan-filovirus RT-PCR. The RADIONE Ebola Detection kit is currently the only available near-point-of-care molecular tool in affected areas that covers BDBV, though formal head-to-head validation against RT-PCR tests still ongoing.
Candidate diagnostics
FIND has undertaken an initial landscaping exercise to map existing and pipeline diagnostic products for Bundibugyo virus, the results of which are published in the FIND DxConnect Test Directory on a rolling basis and inform the landscape described below. FIND, in collaboration with IPPS and as WHO i-MCM-Net Dx Workstream partner, is concurrently conducting manufacturer outreach to identify available and near-ready solutions. To support the assessment of candidates, a BDBV diagnostics validation framework is being prioritised under the leadership of the joint Africa CDC and WHO continental IMST, in collaboration with PATH and FIND, with an expression of interest to follow shortly. This work is supported by Unitaid, which is also working with CHAI to undertake market gap analysis and forecasting, building on the diagnostic landscape. WHO has additionally opened its Emergency Use Listing procedure for in vitro diagnostics for Bundibugyo virus nucleic acid detection; manufacturers are invited to submit a product questionnaire as an initial step, with full EUL submission requirements under preparation.
Molecular – Reference lab based
RealStar Filovirus Screen RT-PCR Kit 1.0 and RealStar Filovirus Type RT-PCR Kit 2.0 (Altona Diagnostics)
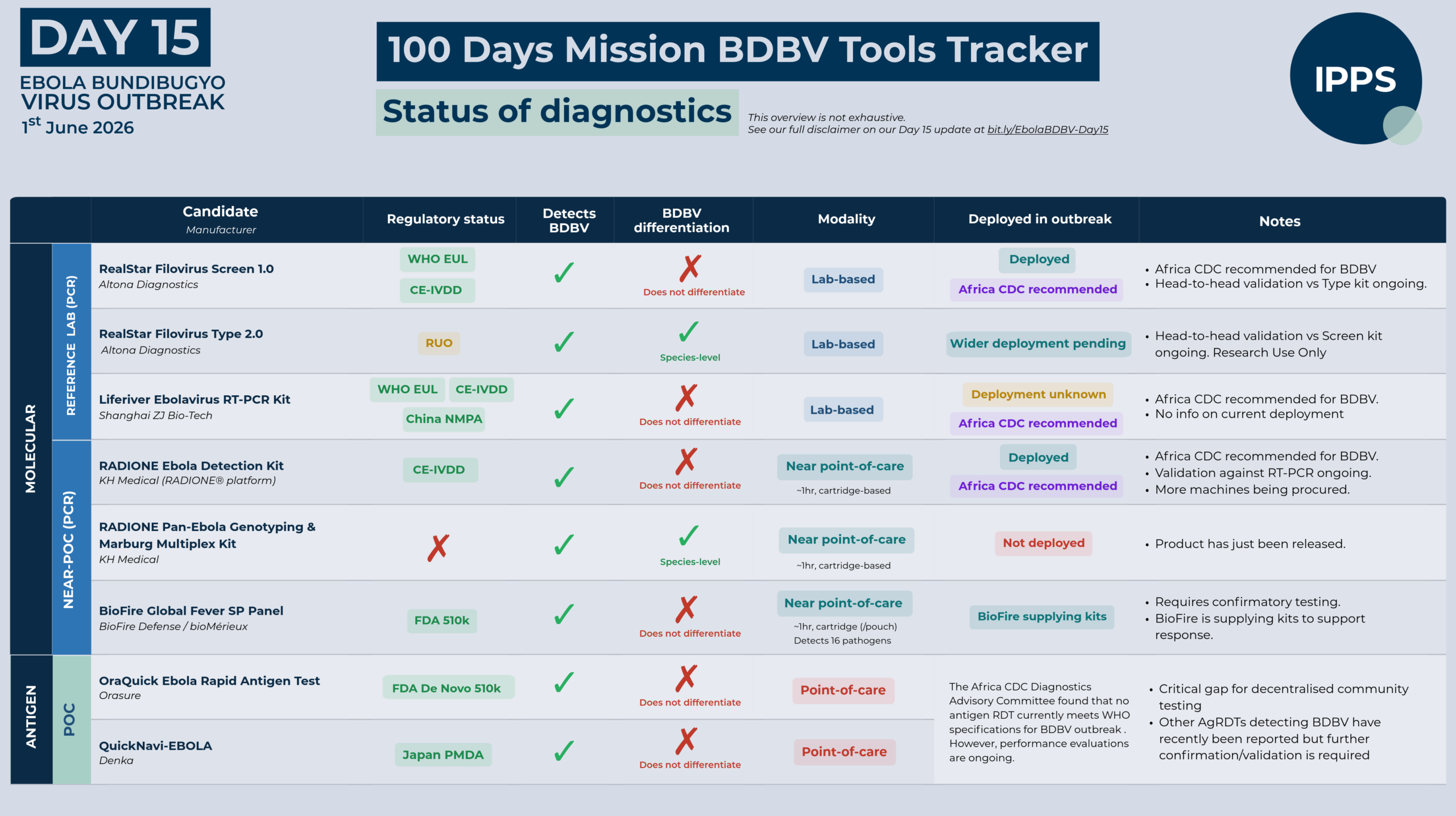
Altona Diagnostics produces three products that cover BDBV, two of which are recommended by the Africa CDC Diagnostics Advisory Committee (DAC) for use in the current outbreak. The RealStar Filovirus Screen RT-PCR Kit 1.0, which holds WHO Emergency Use Listing and CE-IVDD approval, detects and differentiates Ebolavirus from Marburgvirus but cannot differentiate between ebolavirus species; it has been confirmed to detect the circulating Bundibugyo virus. The RealStar Filovirus Type RT-PCR Kit 2.0 additionally differentiates between ebolavirus species, including BDBV specifically, but currently holds Research Use Only (RUO) status; head-to-head validation testing comparing the two kits is currently ongoing. The RealStar Ebolavirus RT-PCR Kit 1.0 (US FDA EUA), also recommended by the Africa CDC DAC, covers BDBV but its regulatory authorisation is US-facing.
Liferiver Ebola Virus RT-PCR Kit (Shanghai ZJ Bio-Tech)
The Liferiver Ebolavirus Real Time RT-PCR Kit holds WHO EUL, CE-IVDD, and China NMPA approval, detects all four pathogenic ebolavirus species including BDBV but does not differentiate between them, and is recommended by the Africa CDC Diagnostics Advisory Committee for use in the current outbreak. No information is currently available on its deployment in the current response.
Molecular – Near point-of-care
RADI Ebolavirus Detection Kit on RADIONE platform (KH Medical)
The RADI Ebolavirus Detection Kit – deployed operationally on the RADIONE platform – holds CE-IVDD approval and is recommended by the Africa CDC DAC for use in the current outbreak. The RADIONE platform is a fully automated, cartridge-based device that integrates nucleic acid extraction and real-time PCR amplification, delivering results in approximately 60 minutes without the need for a conventional laboratory setup, making it suitable for use as a near-point-of-care tool in field settings. However, the kit was not developed specifically for BDBV and cannot differentiate between ebolavirus species; head-to-head validation against RT-PCR reference standards is currently under way at INRB Kinshasa, a process the WHO IHR Emergency Committee has specifically called for. Kits are currently deployed in Bunia; additional reagents and machines are being procured to expand deployment across affected health zones. Of note, KH Medical has recently launched the RADIONE Pan-Ebola Genotyping & Marburg Multiplex Kit, which enables specific detection of BDBV.
BioFire® Global Fever Special Pathogens Panel (BioFire® Defense/bioMérieux)
The BioFire® Global Fever Special Pathogens (GFSP) Panel, which holds US FDA De Novo 510k clearance, is the US CDC recommended diagnostic for the current BDBV outbreak. The GFSP Panel is a fully automated, cartridge-based multiplex assay run on the FilmArray® platform, delivering results from a single whole blood sample in under an hour. It detects all ebolavirus species including BDBV but does not differentiate between them; results are presumptive and require confirmatory testing. Alongside ebolavirus detection it simultaneously screens for 15 other fever-causing pathogens, which has differential diagnosis value in settings where multiple febrile illnesses co-circulate. The ability to quickly differentiate between common febrile illnesses such as malaria and BDBV provides additional clinical utility beyond single-pathogen detection. BioFire® is committed to supplying kits to support the response.
Other point-of-care molecular tests
Through initial landscaping work undertaken by FIND in collaboration with IPPS, one true POC test in late-stage development has been identified, along with six near-POC assays that detect BDBV and are either in late-stage development or at the pre-commercialisation stage. Together, these represent a growing pipeline of decentralised diagnostic solutions that are close to market entry.
Antigen-based Rapid Diagnostic Tests
Antigen rapid diagnostic tests (AgRDTs) have a critical role to play in outbreak response, enabling decentralised testing and faster decision-making at community level. The Africa CDC Diagnostics Advisory Committee reviewed available evidence on antigen RDTs for BDBV against the WHO Target Product Profile for Ebola diagnostics – originally developed in the context of Zaire ebolavirus – and concluded that no antigen RDT currently meets the required specifications for recommendation in this outbreak. However, Africa CDC is planning to conduct evaluations of promising antigen RDT candidates to assess their performance and potential utility during the response.
There are currently six antigen-based RDTs on the market. Of these, OraQuick Ebola Rapid Antigen Test (Orasure) and QuickNavi-EBOLA (Denka) are established products. The remaining four were identified through recent industry surveys and require further verification before formal identification. In addition, five further tests are in late-stage development or nearing commercialisation. All AgRDTS mentioned above are reported by their manufacturers to be capable of detecting BDBV; however, these claims are sometimes based on in silico analysis only, and further validation is required.
Serology
Serology has significant limitations in the acute diagnostic context- antibodies develop too late to be reliable for early clinical diagnosis and are often absent in fatal case. Its primary utility in the current outbreak is in retrospective case ascertainment and seroprevalence surveys rather than acute management.
Therapeutics
On Day 15, there are no approved therapeutics for Bundibugyo virus disease. Existing licensed Ebola therapeutics – Inmazeb® and Ebanga® – are approved for Zaire ebolavirus only and are not indicated for Bundibugyo virus disease. However, a WHO Technical Advisory Group (TAG) has completed a rapid therapeutic prioritisation review identifying promising candidates across two intervention types, none of which have yet been approved or tested in clinical trials for Bundibugyo virus disease.
Prevention through post-exposure prophylaxis represents the most immediately deployable intervention. Obeldesivir – an oral prodrug offering the significant operational advantage of oral administration – has been prioritised for post-exposure prophylaxis in high-risk contacts. Monoclonal antibodies are also being explored for PEP, pending supply availability and alternative routes of administration such as intramuscular injection.
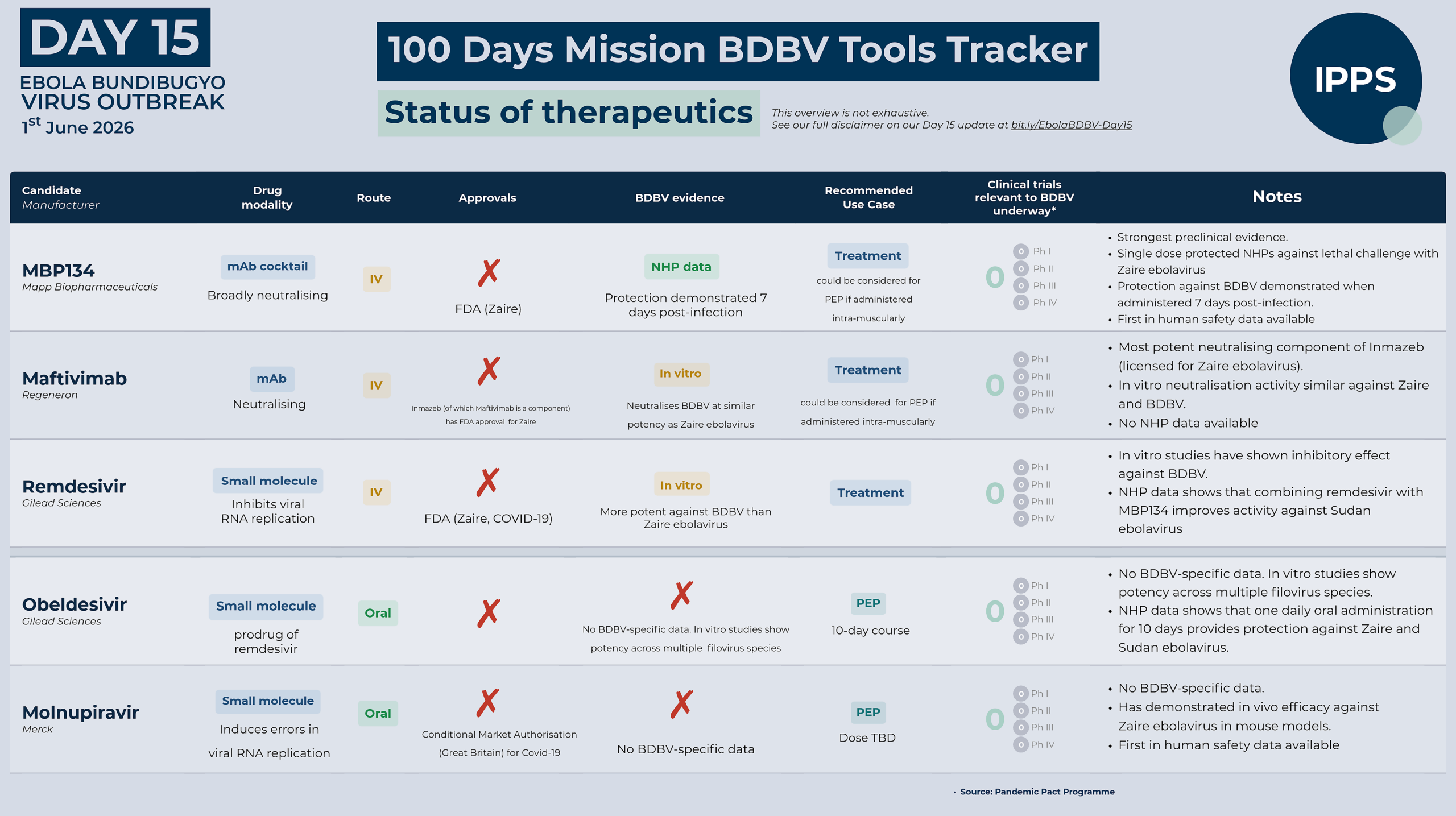
For treatment in confirmed cases, the monoclonal antibody cocktails MBP134 – a pan-filovirus two-antibody cocktail with broad activity across Ebola species – and maftivimab, a monoclonal antibody of interest for its broader activity across Ebola species, have been prioritised alongside the antiviral remdesivir, including the option of combination therapy.
Two clinical trial protocols have been developed to evaluate candidates: PARTNERS, a pan-filovirus adaptive platform trial testing treatment candidates in confirmed cases , and EBO-PEP BUNDI, evaluating obeldesivir and possibly molnupiravir as post-exposure prophylaxis in high-risk contacts. Trials are expected to begin shortly.
Candidate therapeutics
MBP134 (Mapp Biopharmaceuticals)
MBP134 is a two-antibody pan-ebolavirus cocktail comprising two broadly neutralising human antibodies – ADI-15878AF and ADI-23774AF – that target distinct, non-overlapping epitopes on the ebolavirus glycoprotein and have been engineered for enhanced immune effector function. In pre-clinical studies, a single dose protected non-human primates against lethal challenge with Zaire, Sudan, and Bundibugyo ebolavirus. Protection against Bundibugyo was demonstrated even when treatment was administered on day 7 post-infection – at a point when animals were already viremic and showing clinical signs of disease. First-in-human safety data are available, and MBP134 was administered to patients under compassionate use during the 2022 Sudan ebolavirus outbreak in Uganda, though the outbreak ended before efficacy could be assessed in a clinical trial.
Maftivimab (Regeneron)
Maftivimab is one of three monoclonal antibodies in the licensed Zaire ebolavirus product Inmazeb®, and is its most potent neutralising component. It targets a highly conserved region of the ebolavirus glycoprotein – the internal fusion loop – and has demonstrated in vitro neutralisation activity against multiple ebolavirus species including Bundibugyo virus, with similar potency against Zaire and Bundibugyo ebolavirus. Unlike MBP134, no published non-human primate efficacy data against Bundibugyo virus are currently available.
Remdesivir (Gilead Sciences)
Remdesivir is a broad-spectrum antiviral delivered by intravenous (I.V.) administration that works by inhibiting viral RNA replication. In vitro studies have demonstrated that remdesivir exhibits antiviral activity against Bundibugyo that is similar to other filoviruses including Zaire ebolavirus. Importantly, pre-clinical studies in non-human primates have shown that combining remdesivir with the pan-ebolavirus monoclonal antibody cocktail MBP431 significantly improved survival compared with either treatment alone against Sudan ebolavirus, and extended the window during which treatment remained effective. This provides strong scientific rationale for clinical evaluation of a similar combination therapy approach for the Bundibugyo virus. Remdesivir is approved for the treatment of COVID-19 and has been administered made available to more than 14.5 million patients around the world, including more than 8.1 million people in middle -and low-income countries through Gilead’s voluntary licensing programme.
Obeldesivir (Gilead Sciences)
Obeldesivir is an investigational nucleoside analog oral prodrug that generates the same active antiviral metabolite as remdesivir. In vitro studies have demonstrated similar potency across multiple filovirus species including Zaire ebolavirus, Sudan ebolavirus, and Marburg virus. In non-human primate studies, once-daily oral obeldesivir for 10 days provided 80-100% protection against lethal infection with Sudan ebolavirus, Zaire ebolavirus, and Marburg virus when initiated 24 hours after exposure. Obeldesivir has a generally safe and well-tolerated clinical safety profile based on the findings of the Phase 3 OAKTREE trial for COVID-19. Its oral administration offers an implementation advantage for evaluation post-exposure prophylaxis in field settings, and has been prioritised for clinical testing by WHO TAG as well as other stakeholders. Obeldesivir administered as 350mg BID x 5 days was generally well tolerated in >1200 participants with COVID-19 in Phase 3 trials.
Molnupiravir
Molnupiravir is an investigational oral antiviral that works by inducing errors in viral RNA replication. Like obeldesivirit can be administered orally. It has demonstrated in vivo efficacy in mouse models of Zaire ebolavirus infection. Its clinical safety profile is based on its use in COVID-19. No pre-clinical or clinical data against Bundibugyo virus are currently available. It is under consideration as a PEP candidate for the EBO-PEP BUNDI trial alongside obeldesivir, though its dosing regimen for this indication remains to be defined.
Vaccines
On Day 15, there are no approved vaccines for Bundibugyo virus disease. Until recently, two vaccine regimens were licensed for Zaire ebolavirus: Ervebo® and the Zabdeno®/Mvabea® two-dose regimen, which had its European Commission marketing authorisation withdrawn this month.
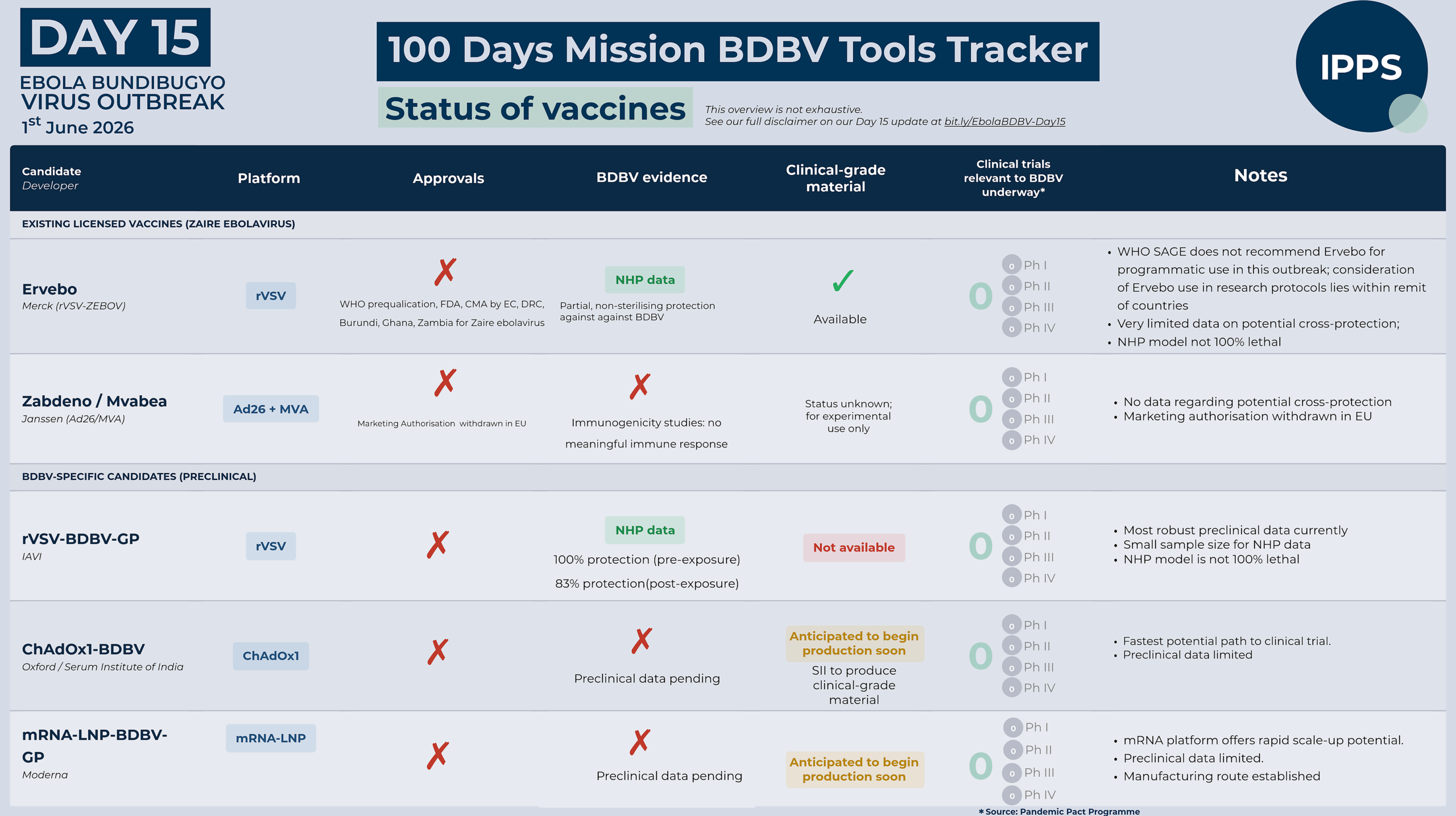
Ervebo® is licensed for prevention of disease caused by Zaire ebolavirus only. There is currently no licensed vaccine available for prevention of disease caused by BDBV. Available evidence regarding potential cross-protection conferred by Ervebo® against BDBV is very limited. No human vaccine efficacy data are available, and findings from the limited number of preclinical studies conducted to date are inconclusive. Overall, available evidence is insufficient to determine or reliably estimate the extent of any cross-protection against BDBV. WHO SAGE consequently recommends that Ervebo® should not be used outside controlled research settings in response to the current outbreak.
Beyond the currently licensed Zaire ebolavirus vaccine, a CEPI-commissioned landscaping exercise has mapped pipeline vaccine products for Bundibugyo virus. This draft mapping informed a WHO Technical Advisory Group prioritisation review. As per the TAG recommendations, the rVSV-BDBV-GP candidate (IAVI) is expected to be the most effective single-dose option for post-exposure use but with an estimated timeline to clinical-grade production of 7 to 9 months and thus may not be an option for evaluation in the current outbreak. ChAdOx1-BDBV (Oxford University/Serum Institute of India) may be the first clinical-grade product to become available, with a two-dose regimen believed necessary for optimal protection. CEPI is funding rapid development of these prioritised candidates and an mRNA-LNP vaccine by Moderna, and has opened a Call for Proposals to evaluate additional promising options.
A prime-boost regimen using investigational rVSV-Sudan and investigational Ebola Zaire vaccines has shown some protection in non-human primates, but these are not licensed products and this approach has no clinical data. The TAG noted that a prime-boost strategy with rVSV-Sudan followed by Ervebo® could be considered for pre-exposure.
Candidate vaccines
rVSV-BDBV-GP (IAVI)
The rVSV-BDBV-GP candidate vaccine, is the most clinically advanced Bundibugyo-specific vaccine candidate in terms of pre-clinical evidence. Using the same rVSV vector platform as the licensed Ervebo® vaccine, it expresses the Bundibugyo virus glycoprotein rather than the Zaire glycoprotein. A single dose conferred 100% protection against lethal Bundibugyo virus challenge in non-human primates, and 83% protection when administered post-exposure (both studies are small sample size, with non-100% lethal model). The post-exposure protection data is particularly relevant in an active outbreak setting where ring vaccination – in which contacts and contacts-of-contacts of confirmed cases are vaccinated to create a protective ring around infected individuals – may be a key deployment strategy. However, no clinical-grade material currently exists, meaning the estimated lead time to a clinical trial is 7 months or more.
CEPI has announced that it will support preparations necessary to generate a Master Virus Seed stock – the starting material needed to manufacture a vaccine – and initiate testing of the seed in an established process using material originally developed at The University of Texas Medical Branch.
ChAdOx1-BDBV (Oxford/ Serum Institute of India)
The ChAdOx1-BDBV programme, led by Professor Teresa Lambe at the Oxford Vaccine Group, uses the same chimpanzee adenovirus vector platform as the Oxford/AstraZeneca COVID-19 vaccine. CEPI is supporting the preclinical testing and development work needed to progress rapidly to Phase 1 trials, as well as creation of a Master Virus Seed stock and manufacturing of clinical-grade doses at the Serum Institute of India. Oxford has indicated the vaccine could potentially be available within 3 months, though this timeline is subject to significant uncertainty and will depend on the results of ongoing pre-clinical studies. No pre-clinical immunogenicity or efficacy data for this specific Bundibugyo candidate have yet been published. However, pre-clinical data from the ChAdOx1-vectored Marburg virus vaccine, when tested against virulent Marburg virus challenge, demonstrate improved survival with a two-dose prime-boost regimen compared to a single dose, suggesting that a two-dose approach might be needed for optimal protection against BDBV. Given the short incubation period of BDBV, a two-dose regimen may not be feasible for post-exposure use, but could provide optimal protection for pre-exposure vaccination in high-risk populations such as health workers and frontline responders.
Beyond the candidates prioritised by the TAG for near-term evaluation, the broader vaccine landscape identified through CEPI’s landscaping exercise includes additional candidates at early stages of development.
mRNA-LNP-BDBV-GP (Moderna)
Moderna is developing an mRNA-lipid nanoparticle vaccine candidate expressing the Bundibugyo virus glycoprotein. Using a platform similar to that deployed for COVID-19, the mRNA approach offers significant advantages for rapid manufacturing and scale-up. The candidate is in preclinical development, and pre-clinical data remain limited. No clinical-grade material currently exists.
CEPI will support preclinical testing and Phase 1 clinical trials, as well as simultaneous manufacturing of doses to enable large-scale Phase 2/3 trials to begin immediately if Phase 1 data supports progression.
Broadly reactive candidates
Beyond Bundibugyo-specific approaches, multiple vaccine candidates are in preclinical development designed to protect against a spectrum of filoviruses, including Bundibugyo virus alongside Zaire ebolavirus, Sudan virus, and Marburg virus.
Given the immediate imperative to respond to the current Bundibugyo outbreak, global prioritisation has appropriately focused on Bundibugyo-specific vaccine candidates, which can be developed and evaluated more rapidly. However, the continued development of broad-reactivity platforms is critical for long-term filovirus pandemic preparedness. These approaches will reduce the need for outbreak-specific vaccine development should other ebolavirus species or filoviruses emerge as future threats.
Calls for Expression of Interest and Proposals
Diagnostics
- WHO Emergency Use Listing (EUL) for nucleic acid detection tests: Manufacturers should submit expressions of interest through the EUL questionnaire.
- FIND Expression of Interest for diagnostic solutions: Manufacturers with candidate diagnostics should participate.
Vaccines
- CEPI Call for Proposals to advance early-stage BDBV vaccine candidates toward Phase 1 evaluation: Developers with scientifically robust candidates on credible pathways to clinical trials are encouraged to apply.
Acknowledgements
We are grateful to the Pandemic Pact Programme, FIND, CEPI, PATH, IFPMA, Roche, MSD, Unitaid, PANTHER Health, Intrepid Alliance, WHO, i-MCM-Net Secretariat, Wellcome, Institut Mérieux, Airfinity, IFPMA and Africa CDC for providing data, verification, and critical feedback that has informed this update.
If you have additional updates or information you would like to see reflected in future iterations, please contact us at info@ippsecretariat.org.
Disclaimer for the Ebola Bundibugyo MCM Tools Tracker
Data shown in the tracker is not exhaustive. It prioritises candidates assessed by WHO TAG, actively discussed in partner coordination meetings and working groups, recommended by Africa CDC, and currently deployed or under evaluation. Additional products and updates will be integrated as they emerge and as existing candidates progress through development and evaluation.